




A new follicular lymphoma CME program worth 1 AMA PRA Category 1 Credits™, is now available on demand. Find it here.
In the Western hemisphere, follicular lymphoma (FL) is the most common non-Hodgkin lymphoma (NHL). In the US in 2018, it is expected that approximately 74,680 new cases of NHL will be diagnosed and 20% of these will be FL. There is no difference across genders, but it appears to increase as age increases. The median age at the time of diagnosis is 60 years and it is rare in adolescents and children. It is twice as common among Caucasians as it is blacks and it is very rarely seen in China and Japan.
FL is considered incurable and often disseminated at the diagnosis. However, it is a slow-growing tumor and highly responsive to current treatments. The median survival rate is 10 or greater years in most patients but most will develop increasing resistance to treatment over time. Additionally, approximately 45% of these patients will convert to an aggressive subtype that is associated with a poor outcome.
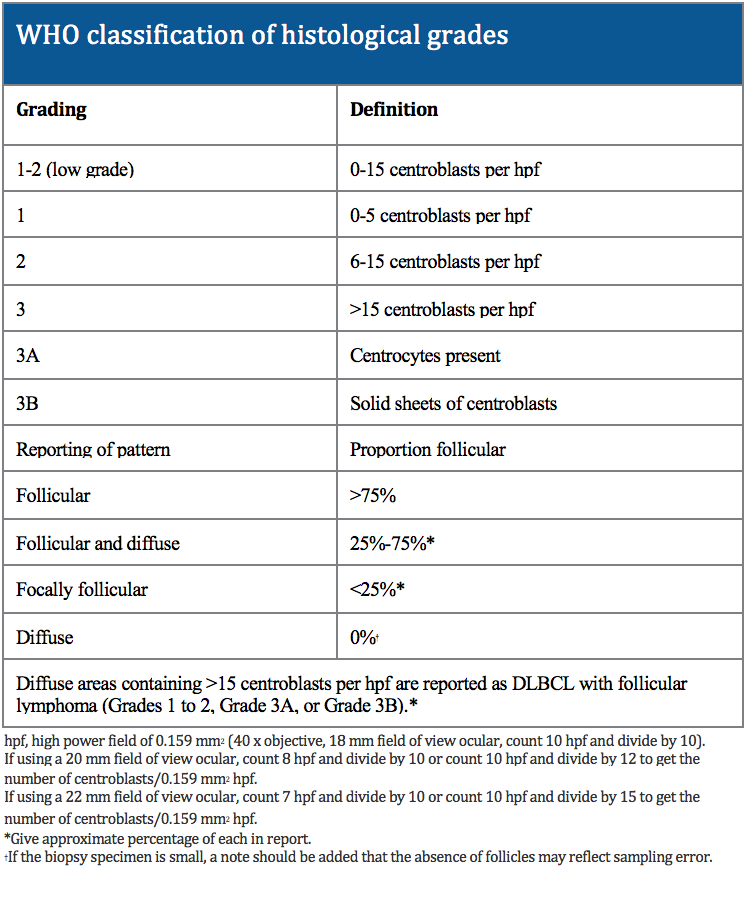
Histologically, FL is marked by proliferation of malignant germinal center B cells mixed with non-malignant cells such as T cells, follicular dendritic cells, and macrophages. Typically, FL is graded based on the number of centroblasts seen in a high power field under the microscope. Higher grades are associated with more aggressiveness while most FLs tend to be low grade.
 During the very early stages of FL, there are no apparent signs or symptoms. Flu-like symptoms such as fever, cough and cold symptoms may be observed. Night sweats, extreme fatigue, anorexia, and unexplained weight loss are typical symptoms. Other possible symptoms include severe or frequent infections, easily bruising, or bleeding, numbness in the hands or feet, headaches, and blurred vision. Sometimes the symptoms will go away only to recur at a later time. On physical exam, lymphadenopathy may be detected.
During the very early stages of FL, there are no apparent signs or symptoms. Flu-like symptoms such as fever, cough and cold symptoms may be observed. Night sweats, extreme fatigue, anorexia, and unexplained weight loss are typical symptoms. Other possible symptoms include severe or frequent infections, easily bruising, or bleeding, numbness in the hands or feet, headaches, and blurred vision. Sometimes the symptoms will go away only to recur at a later time. On physical exam, lymphadenopathy may be detected.
The diagnosis of FL is based on histopathological examination. Typically, immunohistochemical and morphological examination is performed and sometimes flow cytometric and cytogenetic analyses are done as well. FL has a characteristic immunophenotype and B cell markers expressed on the cell surface. The following indices are used: CD20, CD3, CD5, CD10, Bcl-6, Bcl-2, CD21, CD23, and cyclinD1. Additionally, Ki-67 is advised for assessment.
Even in late stages, FL is not life-threatening. It often has a “wax and wane” clinical course. Even with no cure, many patients live eight or more years with advanced disease. Sometimes, FL can undergo a transformation, whereby it becomes aggressive. This transformation can happen in all the cells or just certain parts. If B cells are observed, there is a higher likelihood at transformation. Once it transforms, it is treated like diffuse large b-cell lymphoma.
Much research has been conducted to define the risk factors of FL. One risk factor, other than age, gender, and ethnicity as noted before is the use of certain medications, such as immunosuppressants. This risk has been less definitive with FL than more aggressive lymphomas. Certain viruses, such as Epstein-Barr virus, HTLV, and human herpesvirus HHV-8, have been implication but are more closely linked with diffuse or high-grade lymphomas. Congenital as well as acquired immunodeficiencies have been suspected as well.
Risks factors implicated for FL:
– Age
– Gender
– Ethnicity
– Immunosuppressant medications
– Certain viruses
– Pesticides
– Certain hair dyes
– Tobacco use
– Alcohol use
– T(14;18) translocation
– Genetic alterations at BCL-6
– Epigenetic events
In early stages of FL, observation may be the only treatment needed. External beam radiation is sometimes used when only a single lymph node is affected. Chemotherapeutic agents can sometimes be given alone (fludarabine, chlorambucil, and bendamustine). Comination chemotherapy agents are also used depending on the stage of disease (CHOP, R-CHOP, CVP, and R-CVP). Rituxibam is a targeted agent that can be used in B-cell lymphomas.
Want to learn more? A new follicular lymphoma CME program worth 1 AMA PRA Category 1 Credits™, is now available on demand. Find it here.
About the Author
Linda Girgis MD, FAAFP is a family physician practicing in South River, New Jersey. She was voted one of the top 5 healthcare bloggers in 2016. Follow her on twitter @DrLindaMD.